"Implementation Architect" Framework
Advancing AORN Standards through AI -Enhanced Precision Staffing & Operational ROI
Background:
Perioperative efficiency has traditionally been quantified through time-based metrics, including operating room (OR) utilization rates, surgical case durations, first-case on-time starts, and turnover intervals. OR efficiency is a multifactorial construct influenced by surgical duration, room turnover, staff availability, and equipment preparation (Vladu et al., 2024). Optimizing these parameters particularly punctual start and end times and rapid case turnovers can demonstrably increase surgical throughput (Vladu et al., 2024). However, a sole emphasis on time-based metrics overlooks critical dimensions of system performance. In a systematic review of OR performance optimization metrics, Schouten et al. (2023) concluded that the metrics used to quantify OR performance are highly diverse, that no studies account for possible interactions between metrics of quality and efficiency, and that the well-being of healthcare professionals is underrepresented in current optimization approaches. As surgical volume increases through operational optimization, the cognitive demands on perioperative teams intensify. In recent years, the introduction of new technologies and increasingly complex procedures has generated an overwhelming cognitive load for surgical team members, potentially diluting their attention (Zhang et al., 2024). During complex surgeries, OR nurses must work long hours with high concentration and constant attention to patient safety, exposing them to substantial physical and psychological tension (Teymoori et al., 2022)5. Unmitigated cognitive burden and chronic stress can lead to occupational burnout, which negatively affects patient care, patient safety, job satisfaction, and retention rates (Tolliver, 2025). Burnout-related stress impairs nurses' focus and ability to make sound decisions, increasing the risk of clinical errors; in turn, staff turnover resulting from burnout disrupts continuity of care and places additional strain on remaining team members (Tolliver, 2025). Concurrently, professional organizations have articulated clear guidance on the role of artificial intelligence (AI) in perioperative practice. The Association of periOperative Registered Nurses (AORN) states that "AI cannot and must never be a replacement for the perioperative RN" and that "the human expertise, empathy, and accountability required for clinical decision-making and practice cannot be replicated" (AORN, 2026, p. 1). AORN holds that AI has a complementary rather than replacement role in perioperative care and that, when integrated ethically and responsibly, AI-enabled technologies including machine learning, predictive analytics, natural language processing, and clinical decision support have the potential to optimize workflows, support decision-making, and enhance patient outcomes (AORN, 2026). Similarly, the American Nurses Association (ANA) affirms that AI does not replace a nurse's decision-making, judgment, critical thinking, or assessment skills, and that systems and technologies assisting in clinical practice are adjuncts to, not replacements for, nurses' knowledge and skill (ANA, 2022). These positions highlight the need for practical implementation models that leverage AI to enhance human performance and alleviate cognitive overload while preserving the clinical vigilance of perioperative staff.
Objective:
To evaluate the impact of a staged operational redesign progressing from time-based efficiency improvements to AI-enabled workflow integration on cognitive load, communication efficiency, staffing sustainability, and clinical vigilance within a high-volume perioperative environment.
Methods:
A multi-phase operational improvement initiative was implemented within a hospital-based perioperative setting.
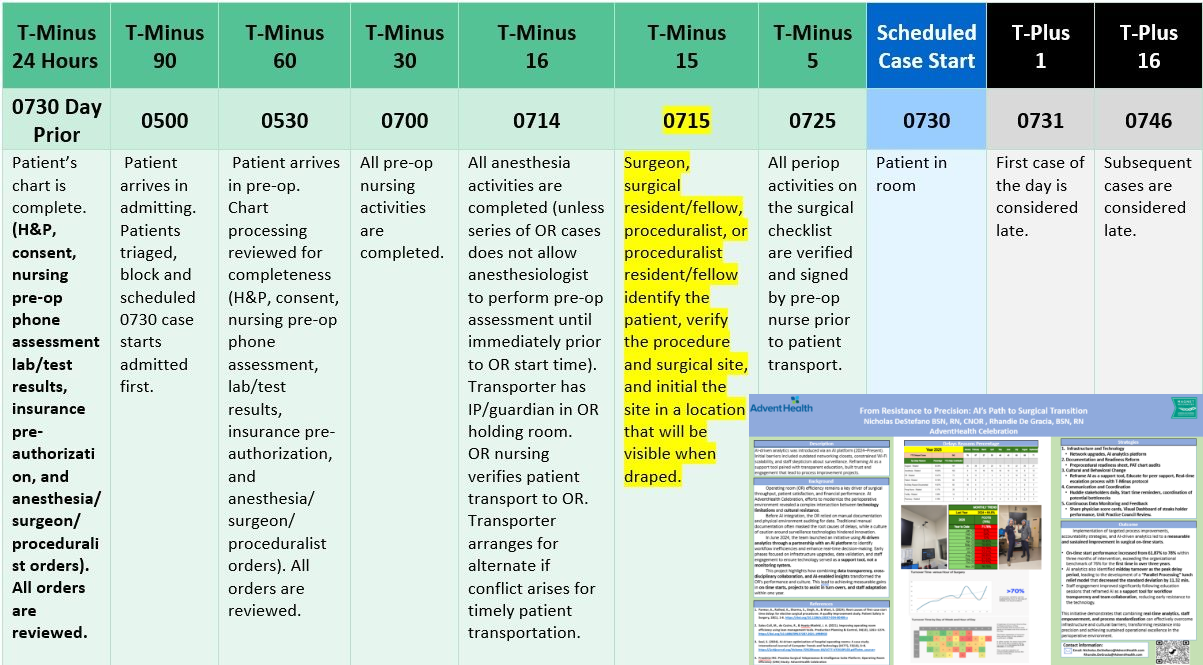
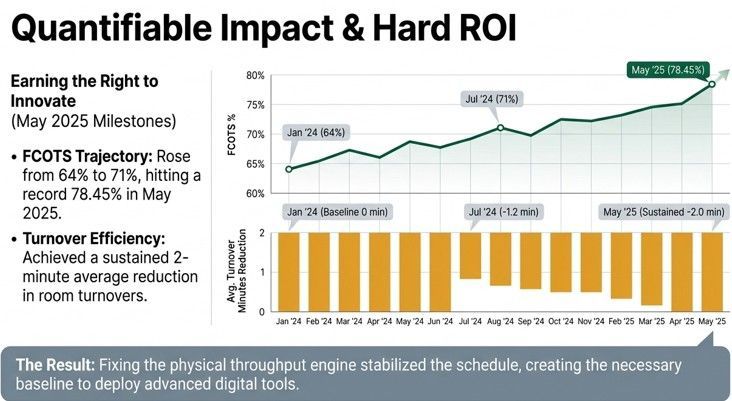
Phase 1 focused on time-based process optimization, targeting improvements in first-case on-time starts and turnover intervals to stabilize daily schedules and increase block utilization. This approach was consistent with evidence demonstrating that systematic strategies for managing surgical start times can significantly enhance OR utilization (Vladu et al., 2024).
Phase 2 introduced structured communication systems. The team established standardized handoff protocols and implemented digital communication tools including secure team messaging via Microsoft Teams and structured electronic handoff forms (Microsoft Forms and Excel) to reduce variability in information exchange. This phase directly addressed the well-documented problem that communication failures are a leading cause of sentinel events in the OR, frequently arising from breakdowns between physicians and nurses (Sillero & Buil, 2021). Multiple handoffs during perioperative care further increase the risk for errors and patient harm (Sparling et al., 2023), underscoring the importance of systematized information exchange.
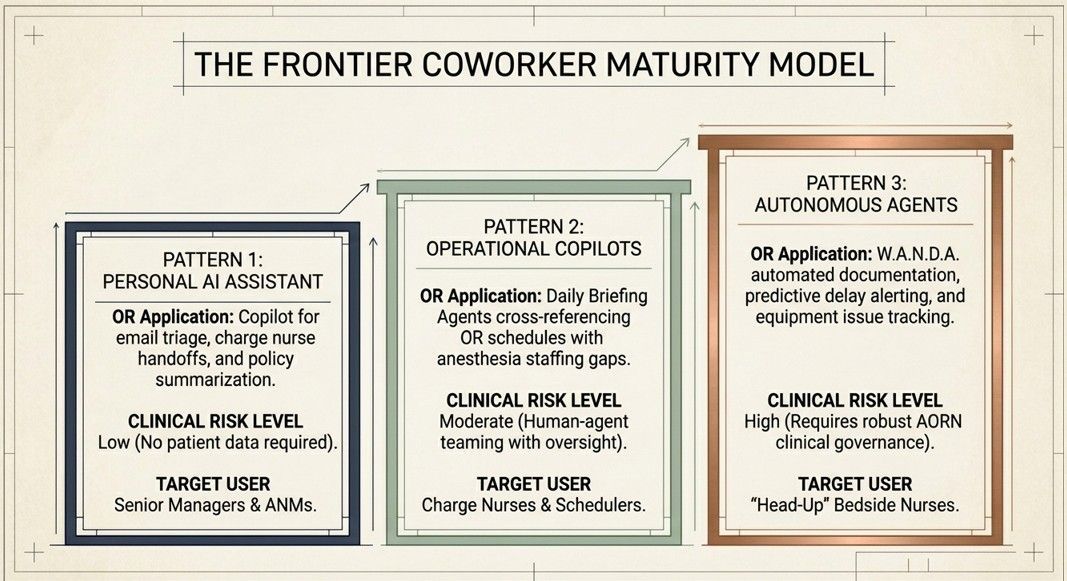
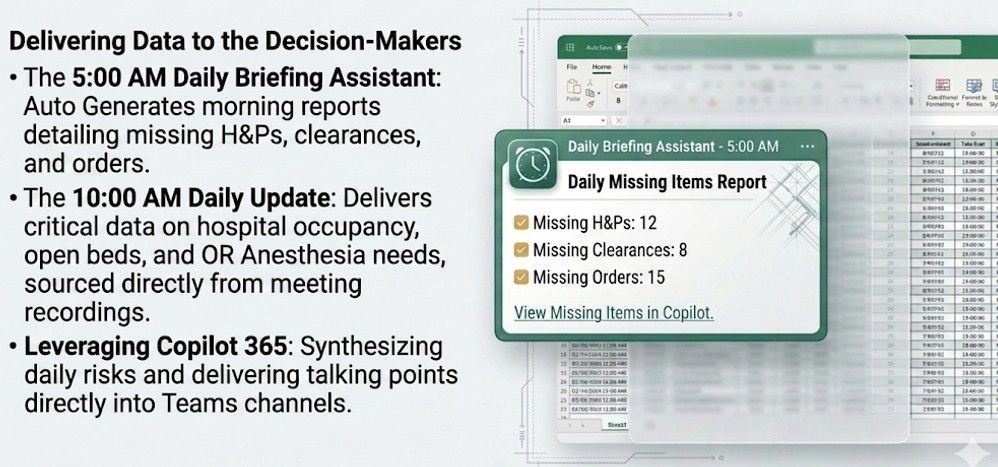
Phase 3 integrated automation and AI-assisted technologies, including Microsoft 365 Copilot and ChatGPT-supported workflow tools, to streamline data capture, analysis, and dissemination. These tools were configured to automatically aggregate operational data including first-case delay drivers, staffing fluctuations (e.g., call-outs), and equipment and supply readiness and generate real-time dashboards and summary reports. Iterative feedback loops were established: insights from the automated dashboards were regularly reviewed by leadership and frontline staff, informing collaborative adjustments to workflows and staffing plans.
Across all phases, data sources included first-case delay logs, staffing variability records, and equipment and supply readiness indicators. The emphasis throughout was on using AI and automation to offload administrative and data-intensive tasks while preserving clinicians' decision-making authority and ensuring that technology outputs remained transparent and easily interpretable consistent with AORN's call for AI systems to demonstrate transparency, explainability, and interpretability to foster trust, accountability, and safe integration (AORN, 2026).
Results:
Phase 1 time-focused interventions improved schedule integrity and enabled an increase in daily surgical volume. Evidence from the literature corroborates this pattern: Vladu et al. (2024) reported that after implementing a structured scheduling algorithm and organizational changes, surgical interventions starting between 8:00 and 10:00 a.m. increased from 28.65% to 32.13% (p < 0.0001), and average OR occupancy between 9:00 and 11:00 a.m. rose from 87.53% to 98.07%. In our setting, the increased throughput from Phase 1 enabled more precise alignment of staffing models and anesthesia coverage with surgical demand.
As operational complexity grew with higher volumes, the communication and automation strategies introduced in Phases 2 and 3 reduced fragmentations in information flow. Implementing a standardized handoff and communication system grounded in the understanding that structured protocols can improve quality and safety of care (Sparling et al., 2023)16 minimized redundant manual updates and the communication breakdowns known to contribute to perioperative errors (Sillero & Buil, 2021). Automating data recording and analytics (e.g., auto-populating delay logs, flagging supply issues, and generating staffing summaries) relieved individual nurses from shouldering multiple manual coordination and documentation tasks. This reduction in repetitive clerical burden was associated with decreased perceived cognitive load among staff and allowed nurses and anesthesiologists to devote more attention to direct patient care and intraoperative vigilance. These observations are consistent with evidence that cognitive support technologies reduce the mental workload of surgical team members and improve overall performance (Zhang et al., 2024) and that digital checklists and cognitive aids reduce cognitive load and improve coordination in high-stress scenarios (Amini Rarani, 2025).
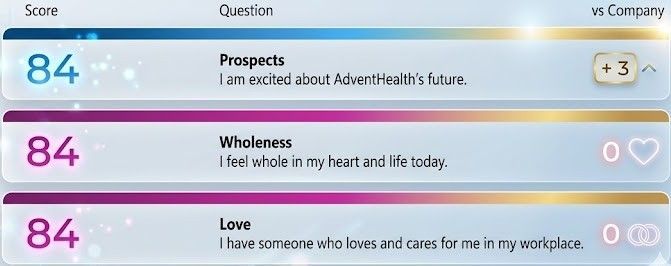
The AI-enabled dashboards enhanced operational visibility and data standardization, facilitating the development of a consistent staffing model across all surgical specialties. The data highlighted predictive staffing variabilities, including patterns in case timing, common late-day staffing bottlenecks, and anticipated gaps due to call-outs or uneven case distribution, enabling proactive staffing adjustments. The department experienced more stable staffing with fewer last-minute reactive coverage changes. These improvements coincided with strong retention outcomes, with voluntary turnover at 3.52% compared with 2024 to 2025 levels that began at 10.3% and ended at 7.7%, supporting the effectiveness of the model. Staff experience metrics also improved, with the hospital Glint survey showing Wholeness at 84%, which was 3 points above the company benchmark, Prospect at 84%, Love at 84%, Wellbeing up 7% from the prior Glint survey to 72%, and Communication up 2%. Together, these findings suggest that workflow redesign and AI-supported operational visibility can improve retention, workforce well-being, and communication while supporting higher reliability in perioperative operations. Improvements in workflow efficiency and reductions in cognitive burden coincided with positive staff retention trends, a finding consistent with the literature demonstrating that reducing excessive workload and stress decreases burnout-related turnover (Tolliver, 2025).
Discussion:
These findings suggest that time-based efficiency gains alone are insufficient to sustain perioperative performance at scale when the cognitive and human-factors' dimensions of system performance remain unaddressed. Schouten et al. (2023) specifically noted that a systems approach is needed to align metrics across different elements of OR performance and that no existing studies account for interactions between quality metrics and efficiency metrics. Transitioning from traditional metrics (e.g., OR minutes, turnaround time) toward attention-based metrics such as Clinical Vigilance Hours, defined here as the proportion of staff time freed for focused patient monitoring, critical decision-making, and intraoperative awareness offers a more comprehensive framework for evaluating system performance. This proposed metric directly responds to the gap identified by Schouten et al. (2023) by incorporating provider cognitive capacity as a measurable outcome.
Automation and AI integration functioned not as replacements for clinical judgment but as mechanisms to reduce cognitive load by consolidating fragmented data streams and eliminating redundant manual review of the same information by multiple staff members. Rather than independently making decisions, the AI tools served as force-multipliers: compiling disparate operational data into succinct summaries and alerts so that clinicians could quickly grasp the operational situation and respond to issues without manually gathering and interpreting all available information. This approach directly operationalizes AORN's position that health care professionals should lead interdisciplinary collaboration in the co-design, implementation, and evaluation of AI systems to reduce cognitive burden, streamline processes, and enhance clinical outcomes and performance (AORN, 2026). However, the benefits of such technologies are tempered by recognized challenges, including alert fatigue, fragmented data systems, and the potential for added digital workload if tools are poorly integrated (Amini Rarani, 2025). This tradeoff underscores the importance of iterative design and continuous feedback from frontline clinicians during implementation a principle reflected in AORN's emphasis on proactive, structured governance and thoughtful operationalization of AI (AORN, 2026).
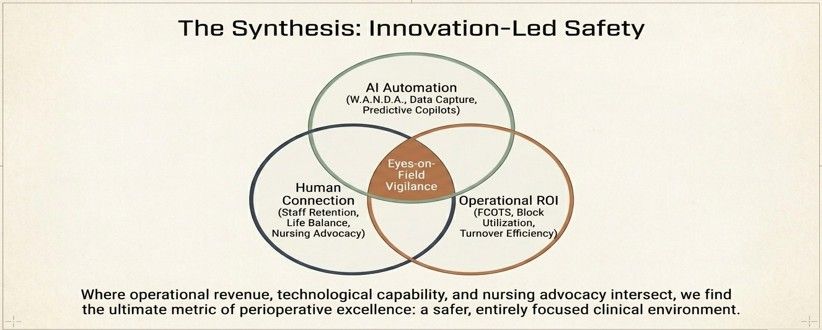
By eliminating repetitious documentation and ensuring critical information was not overlooked amid a busy OR day, the AI-driven automation fostered greater clinical vigilance and teamwork. Staff were enabled to maintain "eyes-on-the-field" awareness of the surgical patient and environment. These improvements in efficiency and information management also created a "staffing dividend": higher throughput and more transparent workflows supported justification for improved staffing models, optimized resource allocation, and workforce sustainability initiatives.
The phased implementation model warrants comparison with other organizational restructuring approaches. Vladu et al. (2024) demonstrated that a computational scheduling algorithm's success was "heavily dependent on the broader organizational changes that were implemented," including standardized team assignments and regular interdisciplinary meetings. This parallel supports the premise that technology alone is insufficient; sustainable improvement requires concurrent organizational redesign. Importantly, the OR environment presents uniquely high cognitive demands. Kennedy-Metz et al. (2022) found that segments of cardiac surgery with the highest percentage of noise peaks (≥10%) were significantly associated with higher team members' heart rates and more case-irrelevant communication events, suggesting that environmental stressors compound cognitive workload and impair effective communication. This evidence reinforces the value of structured communication systems and automation tools that minimize unnecessary cognitive interruptions.
A key limitation of this work is that "Clinical Vigilance Hours" is a proposed metric rather than a validated instrument; further research is needed to develop standardized measurement approaches. Additionally, the generalizability of findings from a single-site implementation warrants examination across diverse institutional settings and patient populations.
Conclusion:
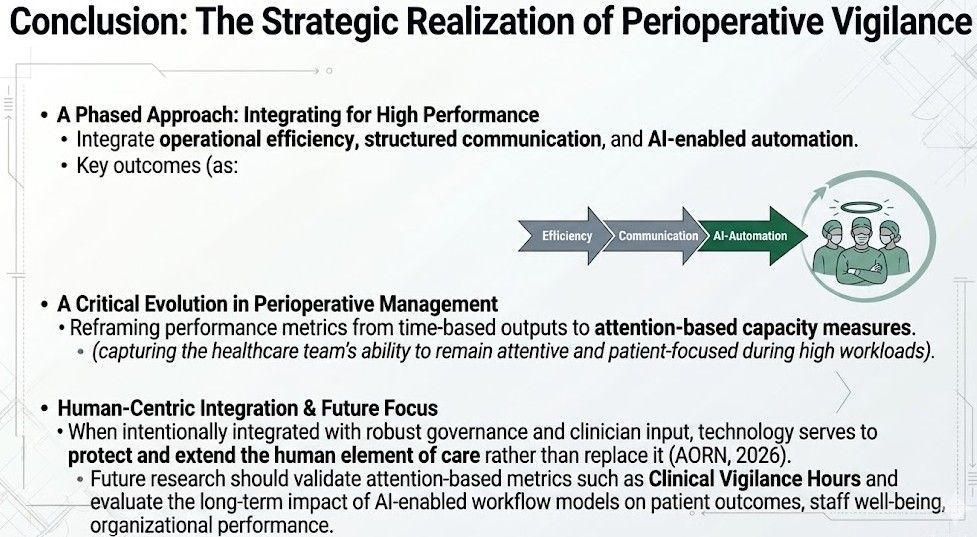
A phased approach integrating operational efficiency, structured communication, and AI-enabled automation can reduce cognitive load, enhance clinical vigilance, and support sustainable staffing in perioperative environments. Reframing performance metrics from time-based outputs to attention-based capacity measures capturing the healthcare team's ability to remain attentive and patient-focused during high workloads represents a critical evolution in perioperative management. When intentionally integrated with robust governance and clinician input, technology serves to protect and extend the human element of care rather than replace it (AORN, 2026). Future research should validate attention-based metrics such as Clinical Vigilance Hours and evaluate the long-term impact of AI-enabled workflow models on patient outcomes, staff well-being, and organizational performance.
Keywords: perioperative efficiency, cognitive load, artificial intelligence, clinical vigilance, staffing models, workflow automation, operating room throughput, nursing retention, healthcare innovation
References
Amini Rarani, S. (2025). Smart technologies and digital innovations for improving perioperative patient safety: A review. Patient Safety in Surgery, 19, 31. https://doi.org/10.1186/s13037-025-00454-y
American Nurses Association. (2022). The ethical use of artificial intelligence in nursing practice [Position statement]. Online Journal of Issues in Nursing. https://ojin.nursingworld.org/table-of-contents/volume-30-2025/number-2-may-2025/the-ethical-use-of-artificial-intelligence-in-nursing-practice/
Association of periOperative Registered Nurses. (2026). AORN position statement on artificial intelligence (AI) in perioperative nursing. AORN. https://www.aorn.org/guidelines-resources/clinical-resources/position-statements
Kennedy-Metz, L. R., Arshanskiy, M., Keller, S., Arney, D., Dias, R. D., & Zenati, M. A. (2022). Association between operating room noise and team cognitive workload in cardiac surgery. IEEE Conference on Cognitive and Computational Aspects of Situation Management (CogSIMA), 2022, 89–93. https://doi.org/10.1109/cogsima54611.2022.9830675
Schouten, A. M., Flipse, S. M., van Nieuwenhuizen, K. E., Jansen, F. W., van der Eijk, A. C., & van den Dobbelsteen, J. J. (2023). Operating room performance optimization metrics: A systematic review. Journal of Medical Systems, 47(1), 19. https://doi.org/10.1007/s10916-023-01912-9
Sillero, A., & Buil, N. (2021). Enhancing interprofessional collaboration in the perioperative setting from the qualitative perspectives of physicians and nurses. International Journal of Environmental Research and Public Health, 18(20), 10775. https://doi.org/10.3390/ijerph182010775
Sparling, J., Hong Mershon, B., & Abraham, J. (2023). Perioperative handoff enhancement opportunities through technology and artificial intelligence: A narrative review. The Joint Commission Journal on Quality and Patient Safety, 49(8), 410–421. https://doi.org/10.1016/j.jcjq.2023.03.009
Teymoori, E., Zareiyan, A., Babajani-Vafsi, S., & Laripour, R. (2022). Viewpoint of operating room nurses about factors associated with the occupational burnout: A qualitative study. Frontiers in Psychology, 13, 947189. https://doi.org/10.3389/fpsyg.2022.947189
Tolliver, N. M. (2025). Elevating well-being and resilience in perioperative nursing: Together we rise. AORN Journal, 121(1), 5–7. https://doi.org/10.1002/aorn.14281
Vladu, A., Ghitea, T. C., Daina, L. G., Țîrț, D. P., & Daina, M. D. (2024). Enhancing operating room efficiency: The impact of computational algorithms on surgical scheduling and team dynamics. Healthcare, 12(19), 1906. https://doi.org/10.3390/healthcare12191906
Zhang, Z. S., Wu, Y., & Zheng, B. (2024). A review of cognitive support systems in the operating room. Surgical Innovation, 31(1), 111–122. https://doi.org/10.1177/15533506231218962
Share